Changing our Healthcare DNA: A Discussion of the Effectiveness of Mammogram Protocols
By Olivia Parlow
For as long as I can remember, I have watched my mother get mammograms. Annually. Religiously. I sat in on appointments. I listened. I watched. Annual breast screenings were embedded into my healthcare DNA. Additionally, I have always been an advocate for preventative care. Screening, testing, you name it. Intuitively it makes sense. The earlier you catch a mass, polyp, or suspicious mole, the earlier you treat it, the better your outcomes will be. So imagine my surprise when I learned that outcomes for patients that received regular mammograms were no different and in some cases, worse, than those that weren’t regularly screened.
Since 1976, the American Cancer Society has recommended mammograms. The first recommendation stated that 40-49 year old women should receive mammograms based on family history of breast cancer and then women over 50 should get screened annually. The United States Preventive Services Task Force is another group that publishes recommendations about breast cancer screening. The first recommendation from the USPSTF was published in 1996 and recommended screening for women ages 50-69 every 1-2 years. Roughly every 6 to 7 years, the Task Force has modified its recommendations as new evidence and research has been released, with the most recent 2023 Draft Recommendation stating that women beginning at age 40 should be screened biennially. This new recommendation is a more aggressive screening protocol compared to the previous 2016 recommendation, which recommended biennial screening for women ages 50-74. In conjunction with a written draft recommendation and draft evidence report, the USPSTF released an informative video to explain the change in recommendation. In this video, they stated their main motivations in altering their screening protocol. This being the significantly higher breast cancer mortality rate amongst black women compared to white women (27.6 per 100,000, compared with 19.7 per 100,000 for White women). While I had previously had my qualms with screening protocols, I decided to take a deep dive into this supposed “new evidence” to see if there was anything compelling that addresses racial inequities within health care as it relates to screening protocols.
Before addressing the 2023 Draft evidence, allow me to introduce my opposition to mammograms. Most research measures screening protocol effectiveness using breast cancer mortality, which is defined by death by breast cancer. A meta-analysis of screening trials indicated that mammograms reduce 8 deaths per 10,000 in women ages 50-59, and 21 deaths per 10,000 in women ages 60-69 (Nelson et al.). However, using breast cancer mortality as a measure of effectiveness disregards an entire chapter of this story. Looking at breast cancer mortality as the sole measure of effectiveness disregards the potential harms of unnecessary radiation treatment, which puts patients at an increased risk of lung and esophageal cancer (Kowalski). A more comprehensive measure of effectiveness would be the all-cause mortality rate. By using all-cause mortality, we ask “Do mammograms prevent women from dying in general?” The answer to this question is no. Using the Canadian National Breast Screening Study, health economist, Amanda Kowalski, analyzed the outcomes of 90,000 women over 20 years and found that “with each additional year that passes after enrollment, an additional 7 excess deaths per 100,000 women become apparent among intervention (screening) arm participants relative to control arm participants.” This is a statistically significant figure that shows that over time, women who were screened annually had a higher rate of all-cause mortality compared to the control group.
Overdiagnosis, which is defined by the USPSTF as “the diagnosis and treatment of noninvasive and invasive breast cancer that would otherwise not have become a threat to their health, or even apparent, during their lifetime,” is the major threat of mammograms that contributes to higher rates of all-cause mortality. Overdiagnosis leads to women being potentially harmed by radiotherapy treatments that can lead to the development of other cancers. Researchers estimate that overdiagnosis by mammograms can be seen at rates between 5 and 55 percent, depending on the subgroup and base rate (Kowalski). To me, the most compelling piece of evidence of overdiagnosis looks at the rates of early stage and late stage cancer overtime as screening protocols became introduced and widely accepted.
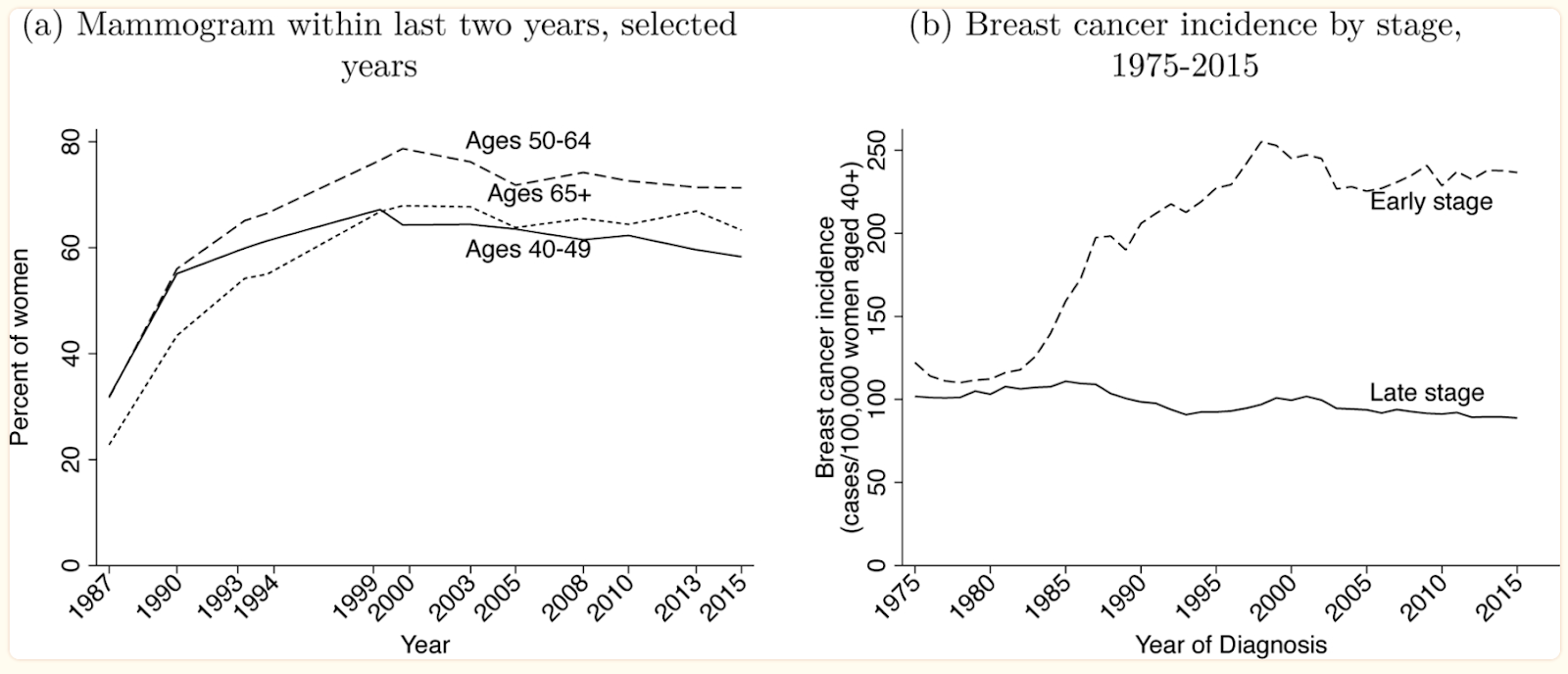
The goal of mammograms is to catch masses early before they develop into later stage, less manageable, more fatal cancers. Therefore, with the introduction and wide adherence to mammogram screening protocols, we expect to see a rise in early stage cancer diagnoses and a decline in late stage diagnoses. However, this has not been the case. A look at breast cancer incidence since the 1980s shows that with the introduction of screening protocols, early stage cancer incidence has drastically increased, but late stage cancer incidence has remained the same (see figure below). This demonstrates overdiagnosis, since screening should detect higher rates of cancer in the short term and lower rates in the long term, but the data tells a different story (Kowalski).
Now that I have provided you with background information on my opinions on mammograms, let me take you with me as I investigate the 2023 Draft Evidence Report. The evidence report was driven by three key questions:
What is the comparative effectiveness of different mammography-based breast cancer screening strategies (e.g., by modality, interval, initiation age, use of supplemental imaging, or personalization based on risk factors) on breast cancer morbidity and breast cancer– specific or all-cause mortality?
Does comparative effectiveness differ by population characteristics and risk markers (e.g., age, breast density, race/ethnicity, family history)?
What is the comparative effectiveness of different mammography-based breast cancer screening strategies (e.g., by modality, interval, initiation age, use of supplemental imaging, or personalization based on risk factors) on the incidence and progression to advanced breast cancer?
Does comparative effectiveness differ by population characteristics and risk markers (e.g., age, breast density, race/ethnicity, family history)?
What are the comparative harms of different breast mammography-based cancer screening strategies (e.g., by modality, interval, initiation age, use of supplemental imaging, or personalization based on risk factors)?
Do the comparative harms vary by population characteristics and risk markers (e.g., age, breast density, race/ethnicity, family history)?
It included 19 studies in its review to answer the aforementioned key questions. Looking at Key Question 1, the review looks at a Finnish study conducted from 1985 to 2007 and assigned participants to either annual or triennial screening. The results concluded that mortality from incident breast cancer diagnoses occurring from ages 40 to 49 (with followup to age 52) was similar between groups, with 20.3 deaths per 100,000 person-years with annual screening invitations and 17.9 deaths per 100,000 person-years with triennial screening invitations. Additionally, all-cause mortality was higher in the annual screening group than in the triennial screening group (21). The evidence that the USPSTF is using clearly does not show immense support for mammograms, but they excuse this because their recommendation is biennial screening and this study analyzes annual and triennial screening procedures. Additionally, the USPSTF stated in their summary of the study’s outcome that “an explanation or mechanism for the higher mortality rate related to more frequent screening could not be identified by the study authors. Deaths from other cancers and deaths from ‘other natural causes’ (not defined) were higher in the annual screening invitation group, whereas deaths from violent causes (accidents, intoxication, murder, suicide) were higher in the triennial invitation group.”
I thought to myself while reading this, “Hmm I could give you a couple reasons. Overdiagnosis and harmful cancer treatment being two of them.”
Being that the new recommendation decreased the age at which to begin screening, one would expect evidence showing that women that begin screening at 40 have better outcomes. However, that is not the case. The report explicitly states that "No randomized trials that assigned individuals to different ages to start or stop screening were identified for inclusion in this review" (40). Once again, the USPSTF is making recommendations without supportive reasoning.
Despite the fact that this new draft recommendation was motivated by racial inequities in healthcare, the report goes on to address that none of the studies included in this review help answer how effectiveness can differ by population (e.g., age, breast density, race/ethnicity, family history), because “nearly all of the included studies were conducted in majority White, non-Hispanic populations and were not powered with adequate numbers of Black, Hispanic, Asian, or Native American/Alaska Native women for meaningful comparisons” (46). So not only are they recommending screening to women at an earlier age, but they are also providing no evidence that shows that increased screening will help women of color or other marginalized populations.
But wait it gets better…
The report once again addresses the inequities in breast cancer incidence and outcomes. It notes that despite Black women having a lower incidence rate of breast cancer, their breast cancer mortality rate is 40% higher than white women. However, Black women also have the highest rate of mammography screening at 84.5%, followed by Hispanic women (79.8%),
Native-Hawaiian/Pacific Islander women (79.7%), Hispanic women (79.8%), non-Hispanic
White women (77.8%), and American Indian/Alaskan Native women (68.7%) (48). This is just another demonstration of how USPSTF’s supporting evidence is contradictory to its recommendations. Instead of calling for more mammograms as a way to address this health disparity, the USPSTF needs to focus on addressing gaps and inequities within healthcare and cancer care.
Every day there is a woman that is faced with the phrase, “It’s time to start getting mammograms.” It has been embedded into our healthcare DNA that this is just another step in womanhood. This concept of getting a mammogram when you reach a certain age has embedded itself into the fabric of women’s healthcare as the norm. So much so that if you question mammograms, or even worse, deny one, you are faced with pushback and liability forms. These guidelines are based on evidence that goes against what groups like the USPSTF are recommending, yet every October women are reminded to get their annual or biennial screening.
Despite the overwhelming amount of compelling evidence against mammograms, I do not see them becoming obsolete. I know that while the high-rate of false positives might be anxiety inducing for some women, the peace of mind of a clear scan will be anxiety reducing for others. I know that there’s an unfortunate truth that the healthcare system is a business and mammograms cost billions of dollars each year. However, what I won’t stand for is using racially motivated reasoning to push for mammograms, when the evidence shows that they do more harm than good. Instead of drafting a more harmful recommendation, the USPSTF needs to draft recommendations that will allow greater access to lifesaving care, as opposed to life diminishing. Additionally, I also hope that more and more people begin to speak about the harms of mammograms, so that women can feel informed and empowered to make the decision that feels best for them, and maybe then, we can alter our healthcare DNA.
Works Cited
Henderson, Jillian, et al. “Screening for Breast Cancer: A Comparative Effectiveness Review for the U.S. Preventive Services Task Force.” U.S. Preventative Services Taskforce, US Preventive Services Taskforce, 9 May 2023, www.uspreventiveservicestaskforce.org/uspstf/document/draft-evidence-review/breast-cancer-screening-adults.
Jørgensen, Karsten Juhl, et al. “Is mammographic screening justifiable considering its substantial overdiagnosis rate and minor effect on mortality?” Radiology, vol. 260, no. 3, Sept. 2011, pp. 621–627, https://doi.org/10.1148/radiol.11110210.
Kowalski, Amanda. “Mammograms and Mortality: How Has the Evidence Evolved?” The Journal of Economic Perspectives : A Journal of the American Economic Association, U.S. National Library of Medicine, 2021, www.ncbi.nlm.nih.gov/pmc/articles/PMC8371936/#R59.
Nelson, Heidi, et al. “Screening for Breast Cancer:A Systematic Review to Update the 2009 U.S. Preventive Services Task Force Recommendation.” National Library of Medicine, Rockville (MD): Agency for Healthcare Research and Quality (US), Jan. 2016, www.ncbi.nlm.nih.gov/books/NBK343819/.

Comments
Post a Comment